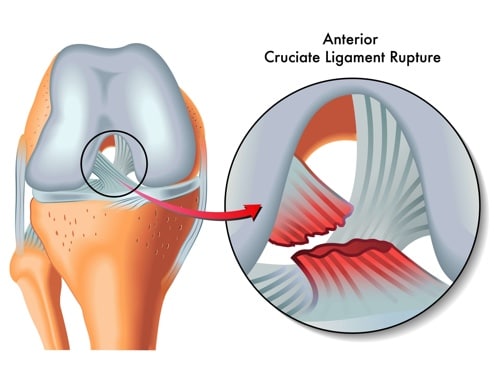
The anterior cruciate ligament (ACL) is one of the 4 large ligaments that hold the end of the femur (thighbone) to the top of the tibia (shinbone). These ligaments limit the movement of the joint so that it remains stable throughout the full range of knee movement. It is approximately 3cm long and about 1 cm in diameter. The ACL prevents the tibia from moving forward on the femur and its close relation, the posterior cruciate ligament (PCL) prevents the tibia moving backwards. Injuries to the PCL are much less common as it is larger and stronger.
The ACL is frequently injured during sporting activity such as football, skiing or following a car or motorbike accident. It is usually injured on its own but may be injured along with the PCL or the other knee ligaments (medial and lateral collaterals, MCL/LCL). Additionally, there may be other damage to the cartilage structures within the knee such as the joint surface or meniscus.
An ACL injury is usually felt immediately, with a sensation of giving way, significant pain and rapid swelling within the first few minutes. It is not usually possible to return to play or “run off” an ACL injury and it is important to seek medical advice soon after injury to reduce any delay to diagnosis or treatment.
Frequently Asked Questions
How is an ACL injury investigated?
Following a detailed consultation and thorough physical examination your surgeon may request additional investigations to help direct your treatment. These may include:
- X-rays to identify the shape and alignment of the bones
- MRI scan to look for ligament or cartilage damage
- CT scan to assess any previous surgery if you have had a previous ACL surgery
Whilst the ACL may sustain a partial tear, similar to a sprain, the usual situation is a complete tear with few or no fibres remaining intact.
How is ACL injury treated?
Once a full diagnosis is made, your surgeon will work with you to formulate an appropriate treatment plan.
Immediate management of an ACL tear involves rest, ice, compression and elevation (RICE) to reduce swelling and enable early physiotherapy which will aid with return of normal range of motion. Depending on your age, activity and desire to return to certain types of sports, ACL injuries may be treated with or without surgery. In general, older patients or those participating in less strenuous sports may be treated with a knee rehabilitation physiotherapy program to regain motion, strength and coordination. Younger patients or those wishing to return to multi-directional sports such as AFL, hockey or soccer may be advised to undergo ACL reconstruction surgery. Where there is additional cartilage or meniscal injury, surgery is usually recommended. Surgery is usually not performed immediately – a delay of a few weeks to allow the initial injury to subside and regain the range of motion has been shown to reduce the risk of knee stiffness after surgery.
What does an ACL reconstruction involve?
ACL reconstruction surgery is most frequently performed by arthroscopic (keyhole) surgery where small cuts are made around the knee to allow a camera and surgical instruments into the knee to assess and treat any injuries inside the joint as well as to prepare the attachment points for the ACL replacement (graft). This is usually formed by taking some of the smaller hamstring tendons from the inside of the leg but other tendons can be used such as the patellar or quadriceps tendon from above or below the kneecap. This is then passed through small holes (tunnels) drilled into the femur and tibia. The graft is then attached to the femur and then secured to the tibia to form a new ACL. The procedure takes approximately 60-90 minutes.
How long will I stay in hospital?
Depending on the procedure, you will usually be able to go home the same day but some patients may stay overnight.
What kind of anaesthetic would I have?
There are various types of anaesthetic techniques used in modern practice and your anaesthetist will discuss which would be recommended in your case. Most patients have a light general anaesthetic and are asleep for their surgery. Different types of pain relief are used in combination after surgery to minimise your discomfort.
What is the recovery period?
You will be mobilising with crutches initially and should be able to fully weight-bear in most cases. A knee brace is not usually required. Regardless of the type of reconstructive surgery performed, it is vitally important that a formal, graduated rehabilitation program is followed with supervision by your physiotherapist and surgeon to minimise the risk of re-injuring the graft. The most important thing to avoid is attempting to return to sports too soon and realistically, most surgeons would recommend not returning to play for 9-12 months after surgery.
What are the risks of surgery?
All surgical procedures can carry some risk and your surgeon will carefully explain these at the time of your consultation.
Does ACL injury re-occur?
It is possible to re-tear an ACL graft but with appropriate surgery and a thorough rehabilitation program this risk is minimised. Returning to sports too soon is a frequent cause of a repeat injury so it is important to take sufficient time to recover from an ACL injury. Additionally, your physiotherapist can take you through a warm-up routine which can be used before sporting activities in the future and this has been shown to reduce the risk of a repeat injury. A knee that has had an ACL injury, even if reconstructed, may undergo wear and tear damage (osteoarthritis) sooner than an un-injured knee.
This page is a brief overview and not designed to be all-inclusive. If you have any further queries, please contact us.



